

What if I told you the solution to safer birth isn’t more monitoring—it’s more relationship?
A continuity of care midwife—the same trusted midwife supporting you throughout pregnancy, birth, and postpartum—might sound like a simple preference. But here’s something that breaks people’s brains: this continuity of care model makes you significantly less likely to need a caesarean section. It makes you more likely to breastfeed. It makes you more likely to actually enjoy giving birth.
Not because of any special intervention. Not because of any new technology. Simply because you know each other. Because trust exists. Because relationship matters.
The medical system doesn’t want you to know this. Because it’s inconvenient. Because it requires them to reorganize how they staff maternity services. Because it centres you instead of institutional efficiency.
But the evidence doesn’t care about their convenience. And neither do I.
The Research They Don’t Tell You About Continuity of Care
When you receive continuity of care from a trusted midwife throughout pregnancy, birth, and postpartum, you are:
- 24% less likely to need a caesarean section
- 19% less likely to need forceps or ventouse
- 16% less likely to experience pregnancy loss before 24 weeks
- More likely to have a spontaneous physiological birth
- More likely to breastfeed successfully
- More likely to describe your birth as positive
- More likely to have shorter labour
These aren’t small differences. These are the kinds of outcome improvements that if a pharmaceutical company discovered them, they’d be celebrated as revolutionary.
But this isn’t a drug. It’s just… knowing your midwife’s name. Being known by them. Building trust over months.
The Studies Worth Knowing About Midwife-Led Care
The Cochrane Review (2016) looked at over 15,000 women across multiple countries. What they found was unequivocal: midwife-led continuity of care produced better outcomes across virtually every measure. Not just “nice to have” emotional outcomes—measurable clinical outcomes. Fewer interventions. Healthier babies. Safer births.
And here’s the kicker: no adverse effects. None. Continuity of care is safer and more satisfying.
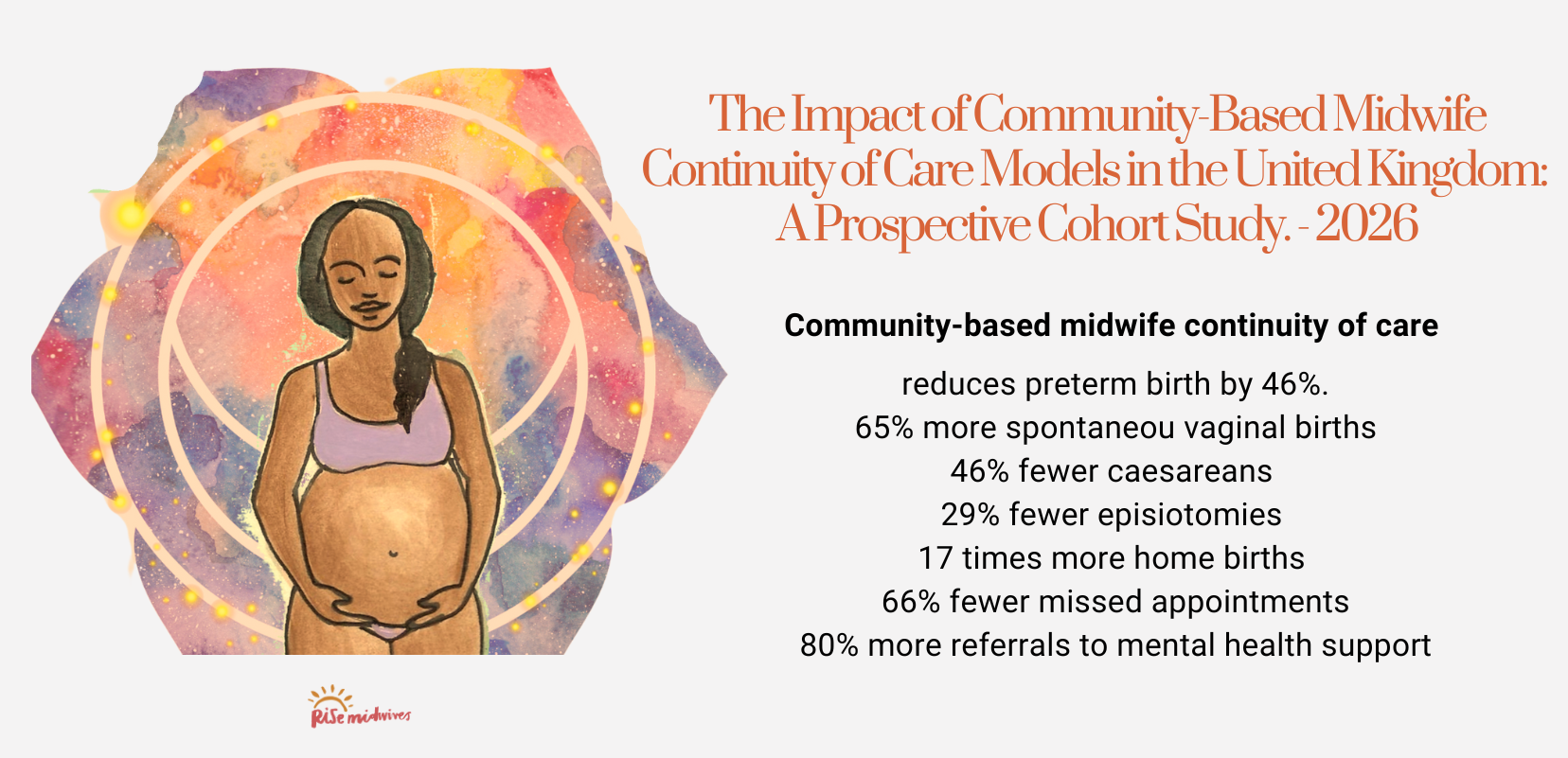
A groundbreaking 2026 study published in BJOG followed 6,690 pregnancies in South London between 2018-2020, examining community-based midwife continuity of care models for women living in socially disadvantaged and ethnically diverse areas. The findings were clear: women who received continuity of care experienced significant improvements in birth outcomes. This matters profoundly because these populations often face the highest intervention rates and poorest maternity outcomes under standard fragmented care models. Continuity of care doesn’t just work for the privileged—it works especially well for those who need it most.
A 2024 systematic review confirmed these findings still hold. Across different populations, different healthcare systems, different countries—the pattern is consistent. Relationship-based care works.
The Royal College of Midwives advocates for continuity of carer as best practice, recognizing that this model produces the best outcomes for birthing people and babies.
Why Does a Continuity of Care Midwife Model Work? Let’s Talk Biology
Birth isn’t a mechanical process that happens to you. Birth is a hormonal, relational, deeply embodied experience that you move through.
And here’s what matters: your nervous system knows the difference between feeling safe and feeling observed by strangers.
Oxytocin Needs Safety
When you feel safe, held, trusted—when you’re with someone who knows you—your body produces oxytocin. This is the hormone that powers contractions, helps your cervix open, facilitates birth, enables bonding, and supports breastfeeding.
Ina May Gaskin says it beautifully: “Love and gratitude are inextricably intertwined. When they flow together, the oxytocin levels in the birthplace may rise and offer incredible possibilities for transformative moments.”
But when you’re labouring in a hospital with strangers rotating through your room every shift change? When you’re being observed rather than held? Your body produces adrenaline and cortisol. Stress hormones. And these hormones actively slow down labour.
This isn’t woo. This is physiology. Your body is designed to labour best when you feel safe. And you feel safest with people you trust.

How Your Midwife’s Knowledge Prevents the Cascade of Intervention
Here’s what happens with fragmented care: a midwife you’ve never met walks into your room, looks at your notes for 30 seconds, sees your blood pressure is slightly elevated, and makes a decision based on protocols and risk aversion.
Here’s what happens with continuity of care: your midwife, who has known you for months, knows that your blood pressure runs slightly higher when you’re anxious. She knows you’re terrified of needles. She knows this is normal for you. She can distinguish between variation and genuine concern.
That knowledge prevents unnecessary intervention. It prevents the cascade that starts with “just to be safe” and ends with forceps, or caesarean, or trauma
What a Continuity of Care Midwife Actually Provides
This isn’t theoretical. This is what I offer through Rise Midwives—and what I believe should be available to every birthing person.
Care That Begins With Relationship
Your first appointment isn’t a 10-minute box-ticking exercise. We take as long as we need—usually 90 minutes or more. Because I need to know you. Your history, yes. Your medical background, absolutely. But also your hopes, your fears, what makes you feel strong, what makes you feel small. What happened to your mother during her births. What you’re carrying that you haven’t told anyone.
This is where trust begins. Not in the birth room—here, in early pregnancy, when we have time.
Appointments That Actually Have Space
Throughout your pregnancy, we meet regularly—monthly until 24 weeks, then fortnightly. Each appointment lasts about an hour. Not because I’m slow, but because we’re doing more than measuring your bump and listening to heart tones (though we do that too).
We’re checking in with your emotional wellbeing. We’re exploring whatever you need to explore—birth fears, feeding worries, relationship changes, what your body is telling you. We’re addressing pregnancy discomforts using aromatherapy, positioning, breath work, or whatever feels right for you. We’re navigating the maternity system together—what tests you actually need, what choices you’re facing, how to advocate for yourself.
We’re preparing for birth in ways that go deeper than “breathing techniques.” We’re talking about what you need in your space, who you need with you, what makes you feel safe. We’re addressing the fears that live in your body, not just your mind.
And we’re preparing for the fourth trimester too—because the support you need doesn’t end when the placenta is born. We talk about feeding your baby (however you choose to do that), about attachment, about what you’ll actually need during your babymoon, about realistic expectations so you’re not blindsided by the intensity of early parenting.
Support That Doesn’t Clock Off
You also have my phone number. Monday to Sunday, 9am-8pm. Because questions and worries don’t only arise during business hours. Because at 11pm when you’re bleeding slightly and don’t know if it’s normal, you shouldn’t have to call 111 and speak to someone who doesn’t know you.
The Home Birth Evidence with Continuity of Care Midwives
When a continuity of care midwife supports your choice to birth at home, the outcomes become even more striking:
- 40% less likely to have caesarean
- 50% less likely to need forceps or ventouse
- 70% less likely to request epidural or other pain medication
- 60% less likely to need synthetic oxytocin
- 100% more likely to describe your birth as empowering
These numbers come from the Birthplace Study—one of the largest, most rigorous studies of birth place ever conducted. For healthy women with straightforward pregnancies, planned home birth with a known midwife is at least as safe as hospital birth, and by many measures safer.
Why don’t they tell you this? Because it’s inconvenient. Because hospitals are set up for hospital birth. Because the system profits from intervention, not from supporting physiology.

Transactional Care vs Relationship-Based Continuity of Care
Let me paint you two pictures.
Fragmented care looks like this: Brief appointments with whoever is available. Different face at every visit. Hospital-based birth with rotating staff. Meeting the person who will catch your baby when you’re already 6cm dilated and in active labour.
This model treats birth as a medical event requiring surveillance. You are a uterus with a problem to be solved. Your care is efficient, protocol-driven, risk-averse.
A continuity of care midwife model looks like this: The same midwife throughout. Someone who knows that you process information slowly and need time. Someone who remembers that your sister had a traumatic birth and it’s affecting how you feel. Someone who knows what questions keep you awake at 2am. Someone who has earned your trust over months, not minutes.
This model treats you as a whole person moving through transformation. Your midwife knows not just your medical history but your story. And that knowledge lives in relationship—it can’t be documented in notes and passed between strangers.
This Should Be Normal, Not Radical
Here’s what makes me angry: continuity of midwifery care produces better outcomes across every single measure. It’s safer. It’s more satisfying. It prevents intervention. It supports physiology.
And yet it remains rare in most NHS trusts. Though the NHS recommends continuity of carer, the system prioritizes institutional efficiency over relationship. Because it’s easier to staff shifts than to reorganize around continuity. Because medical culture still treats birth as inherently dangerous rather than inherently powerful.
So independent midwifery exists in the gap between what the evidence shows works and what the system actually provides.
Your Birth Deserves a Continuity of Care Midwife
If you’re pregnant or planning pregnancy, I want you to ask these questions of your maternity care provider:
- Will I see the same midwife throughout my pregnancy?
- Who will attend my birth—someone I know, or whoever is on shift?
- Will I receive postnatal care from someone who already knows my story?
You deserve care that sees you as a whole person. You deserve someone who knows your name, remembers your fears, celebrates your strength. You deserve relationship-based care.
Not because it’s “nicer” (though it is). Because the evidence shows it produces better outcomes. Because your body labours best when you feel safe. Because trust unlocks biology.
Finding a continuity of care midwife who offers this relationship-based model can transform your entire birth experience.
If you’re ready to explore what continuity of care looks like with Rise Midwives, book a free discovery call and let’s talk about your journey.
Changing birth means changing how we care for women and birthing people. And that starts with relationship.
References
- Sandall, J., et al. (2016). Midwife-led continuity models versus other models of care. Cochrane Database of Systematic Reviews. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD004667.pub5/full
- Birthplace in England Collaborative Group. (2011). Perinatal and maternal outcomes by planned place of birth. BMJ, 343. https://www.bmj.com/content/343/bmj.d7400
- Homer, C.S.E., et al. (2024). Continuity of midwifery care: Updated systematic review. BMC Pregnancy and Childbirth. https://bmcpregnancychildbirth.biomedcentral.com/articles/10.1186/s12884-024-06969-w
- Fernandez Turienzo, C., Burton, S., Khan, Z., et al. (2026). The Impact of Community-Based Midwife Continuity of Care Models for Women Living in Areas of Social Disadvantage and Ethnic Diversity in the United Kingdom: A Prospective Cohort Study. BJOG, 0, 1-16. https://doi.org/10.1111/1471-0528.70101





